
Publications & Presentaions
BREAST ENLARGEMENT
Download BREAST ENLARGEMENT.pdf
Why and when is a Breast Enlargement performed?
The size of a woman’s breast will largely be determined by genetics but it will also be influenced by fluctuations in weight, pregnancy, breast feeding and hormonal changes
Some women have problems with asymmetry (one breast much larger than the other). Others have very small breasts, breasts that are out of proportion for their frame or breasts that decrease in size after pregnancy. Surgery would not usually be offered to a teenage girl whose breast might not have reached full maturity.
What is involved in the Operation?
Breast enlargement surgery will usually be performed under a general anaesthetic, takes one to two hours and in some cases might be performed as a day case without the need for an overnight stay in hospital. The surgery involves placement of an implant either under the skin and breast tissue or deeper under the muscle under the breast. There are many different types of implant available. They all have a silicone outer layer but may be filled with silicone (cohesive gel that doesn’t run if cut), saline (salt water), oils or a combination of these. The choice of implant should be discussed with your surgeon and the position of the scars should also be discussed. There are different techniques available which result in different scars either under the breast, around the nipple or in the armpit.
Before the operation, depending on your age and fitness, you may have to undergo some simple health checks such as blood tests and a mammogram. If you decide on surgery you will be required to sign a consent form giving permission for the operation. This requires that you are aware of the risks and complications involved with the procedure.
Are there any Complications?
There are general risks associated with a general anaesthetic including chest infection and DVTs (clots in the veins of the legs). There are risks specific to breast surgery.
Bleeding, sometimes requiring a return to theatre, and problems with wound healing and infection can occur particularly in those who smoke and it is therefore advisable to stop smoking before the operation. In some cases infection might result in the implant having to be removed. In most cases the scars will fade and be hardly noticeable and would not be visible in normal underwear or swim wear. Scars vary enormously from one woman to the next and some people can have problems with red, raised, and lumpy scars. Internal scarring around the implant, known as a capsule, occurs to some extent in up to 10% of women. In the worst cases this leads to hard painful breasts and may require further surgery. Asymmetry (one side different in size or shape) can occasionally be a problem as can numbness or altered sensation. Rupture or leakage of the implant is rare. Despite media reports, there is currently no convincing evidence linking implant to increased risk of breast cancer or other health problems such as auto-immune diseases and rheumatoid arthritis. It is possible to have mammograms after breast enlargement surgery and it may also be possible to breast feed in many cases.
What happens after the Operation?
After the operation there will be swelling and pain and you will be advised to take pain killers and wear a supportive bra day and night. You may have dissolvable stitches but any permanent stitches will need to be removed at around 10 days.
When can normal activities be resumed?
You should avoid lifting, driving and strenuous activity for up to 3 weeks. Depending on your job, you should be able to return to work 2 to 4 weeks after the operation.
THE RICE TEST
Introduction
The Rice Test is designed to help us both understand what sort of breast volume you are hoping to achieve following your augmentation. It is difficult to imagine how you might feel with a C or D cup and how this would look in either a bra or your normal clothes. Doing the test is a very important part of this process. It might sound silly and you might feel silly but it helps you to pinpoint exactly what you are aiming for, and helps us to understand how you feel.
It is also difficult to surgically provide to an exact cup size. However, the implants are measured by their volume and by doing this simple test we can work out what size implants are right for you.
Doing the Test
This test is most easily done with rice, however, you can use other things such as couscous or tapioca or even sugar if you like. First use a measuring jug and fill with uncooked rice 250cc/ml is a good place to start. Pour the measured rice into a plastic bag, ensuring that the bag is big enough to allow the rice to spread out, and seal the bag. Repeat with a second bag. Put on a bra of the size that you think that you would like to be wearing after your surgery. Then put the sealed bags inside your bra and carefully smooth the rice until the cups are filled appropriately. Change the amount of rice until you are happy that the bra is nicely filled and you have achieved the result you would like with a reasonably tight top on. Now measure the final volume of rice and bring the information to your next consultation.
What happens next?
The volume that you have measured doing the Rice Test and the measurements taken of your ribcage are used to calculate the implant that is likely to achieve your desired volume. This is the start point for your augmentation. It does, however, only provide part of the overall picture and during your surgery a sizing implant system is used to check the appearance of the proposed implant and the final implant size and shape is then selected. Every patient is different and we tailor your augmentation to reflect both your current shape and the shape you would like to be. It is very important that Miss Cubison fully understands the size and shape that you would like, so that we can achieve the result that you are looking forward to.
OPERATIVE SEQUENCE – WHAT WILL HAPPEN AND WHEN
First Consultation
Your first consultation is an opportunity to find out whether an augmentation is suitable for you and to help us to start to identify which type of implant would give you the result that you are looking for.
We usually cover issues such as types of implant and their placement, and the scarring that you can expect.
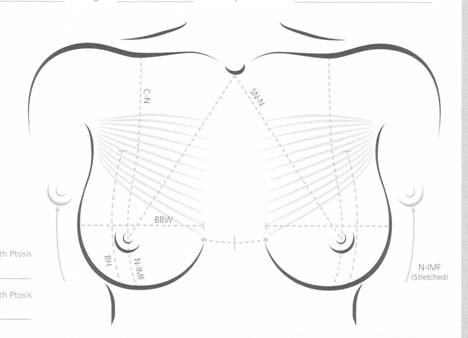
You will be examined and measured, and photographs will be taken. At the end of the appointment you will be asked to perform the Rice Test at home and to bring the information to your next consultation.
This first appointment is very important to try and understand the look you are trying to achieve, so that we can identify the type of implant that will be best for you.
Second consultation
The second consultation will normally happen two weeks after your first consultation and at least two weeks before your proposed date for surgery.
At your second consultation we will review the results of your Rice Test and talk in more detail about the risks and complications of implant surgery.
At the end of this consultation you should be ready to proceed with surgery if that is what you have chosen to do.
Subsequent consultations
Should you feel that you require more time to think about the situation or have further questions to ask we would be happy to arrange further consultations as necessary.
Pre-assessment
In certain situations, particularly if you have other medical problems, it may be necessary for you to attend a pre-assessment visit prior to your operation. At this visit the nurse practitioner will assess you and arrange any necessary investigations such as a heart trace or blood tests. This is important to ensure that your anaesthetic is as safe and trouble free as possible. The pre-assessment team will contact you directly to arrange this if required.
Your Admission
Unless there are special circumstances you will be admitted to the Ward of the McIndoe Surgical Centre in East Grinstead on the morning of your surgery. The Hospital will send you an Admission Pack, with information about your admission time etc, and may ask you to ring and confirm that a bed is available the day before. If your operation is scheduled for the morning you will be asked to not have any breakfast and you will be given a time at which you must stop drinking even clear fluids. If your operation is in the afternoon you are likely to be asked to have a light, early breakfast and then to drink for a further period of four hours after you have completed your breakfast.
Please ensure that you read your Pack carefully as starvation times are an important safety issue and if you do not follow them carefully your surgery may have to be rearranged as it would not be safe to anaesthetise you.
Please bring with you a comfortable sports bra or two in the size that we are hoping to achieve. These should not be expensive ones as they may be stained after the surgery. The bra should have adjustable back fitting and adjustable over-the-shoulder straps.
Before surgery you will meet your anaesthetist and Miss Cubison will go through the Consent Form process with you.
Your operation will take approximately 2 hours, after which you will wake up on the recovery ward before returning to your room. You will be watched carefully by the nursing staff and observations will be done, including the volume of fluid collecting in your drains.
You will normally stay overnight for 1 night before your wound drains can safely be removed.
Post op day 1
Miss Cubison will visit you early on the day after surgery normally between 7 and 8 o’clock to check that all is well and that the drains are ok. Once the drains have been removed you can go home (around lunchtime) if you are comfortable to do so. To get home you will normally need to ride in a car and it is advisable to bring a soft pillow to place under the seatbelt for your journey home. You cannot drive yourself home from hospital.
It may be necessary for you to remain in hospital for a further night if you are uncomfortable or there has been too much drainage in the first 24hours.
At home
During your first week you will need to rest at home, doing minimal physical activity and wearing your sports bra night and day. You can bath or shower but should ensure that the brown tape covering your scars is patted dry or dried with a hairdryer on a cool setting to ensure that you do not have a soggy dressing in contact with the wound surface for any length of time. Your wounds will normally be checked at 1 week after your surgery, either by the nursing team at the McIndoe Surgical Centre dressing clinic, or by Miss Cubison herself at an Outpatient Clinic. Although your stitches will be dissolving there may be an outside stitch at the end of the wound which will be trimmed at your first follow-up visit.
Levels of Activity
For the first week you should rest, stay at home, and potter gently. It is best to make alternative arrangements for childcare and do not undertake any sporting activity.
For week two you can walk about, do light normal tasks. Don’t carry shopping or children, or full A4 files of paper. But you can do washing up, ironing, photocopying and typing.
For week three you can start light activity eg, swimming (if the wounds are healed), exercise bike, and most standard office or domestic activities.
If it hurts DON’T DO IT!
Wear the sports bra night and day for six weeks to ensure the intended breast shape is maintained and for comfort. Your breasts will be heavier – they will need more support than you are used to. You will find underwired bras will be most uncomfortable for the first couple of months – although they look good they are likely to rub on your scars. It is quite acceptable to wear an underwired bra for a short period for a special event – but take a sports bra with you in case you get uncomfortable.
IMPLANT SELECTION
What are implants made of?
All implants consist of a shaped silicone bag, full of either silicone gel or another substance. The most common fillers are saline solution, different forms of silicone gels and other gels such as soya and hydrocoloid gel.
Saline
Saline implants are empty silicone bags filled with salty water which can be filled up after they are put inside. These are especially useful if your skin is very tight or you have breasts of different sizes that are still growing. The problem with saline implants is that if they rupture they completely deflate (loose all the saline and therefore all the benefit) and some patients can feel the fluid moving around inside them.
Silicone Gel
Silicone is a substance that has been used since the 1960s to fill breast implants and also to make a number of other medical products used within the body. It comes in a number of forms from a plastic fabric used to make the shell for the implant to various thicknesses of gel to fill the implant with. The soft gel is like a thick syrup which has a consistency of normal fat and therefore feels the most natural to touch and is most comfortable to lie on. It finds its own shape within the implant shell and provides a very natural shape in all positions. However, if the shell ruptures the gel will come out into the surrounding scar capsule. It is very unusual for the silicone to escape further than the surrounding scar capsule and this is a small risk only.
Implants are also sometimes filled with a thicker Cohesive gel which is rather like the inside of a jelly baby – it does not pour out if opened. However, this is harder to touch and lie on and keeps a definite shape within the implant. The thicker gel is often used to create more fullness in the upper part of the breast if we are trying to achieve a more “implanted” look with a more pronounced cleavage. The Cohesive gel is often used in a shaped implant and if these are used there is the risk that they can rotate and give an unsatisfactory result.
Is Silicone safe?
A number of years ago in the USA, a small group of women reported problems after breast augmentation with silicone implants. These included joint problems and general aches and pains. The USA government immediately banned the use of silicone implants while this was investigated. These implants were not banned in the UK and we continued to use them here. After a significant amount of careful research it was decided that silicone implants did not increase risks of joint problems etc and they are now available again in the USA. There is lots of detailed information available about these studies on the internet and if you would like to read more about this please go to www.mhra.gov.uk for more details. Miss Cubison has read much of the available information and is happy that silicone implants are the best option for the majority of her patients.
Other Gels
Due to concerns about the safety of silicone (now refuted) a number of other oils were developed for use in breast implants. These include soya oil and hydrocolloids. Unfortunately these have also had problems with leaking, and some gradually took in fluid and became larger over time. Many of these alternative implants have now been withdrawn from the market and a number of patients have had to have implants removed for safety reasons. Miss Cubison does not use these products as she believes that silicone gels have the best profile of safety and cosmetic result.
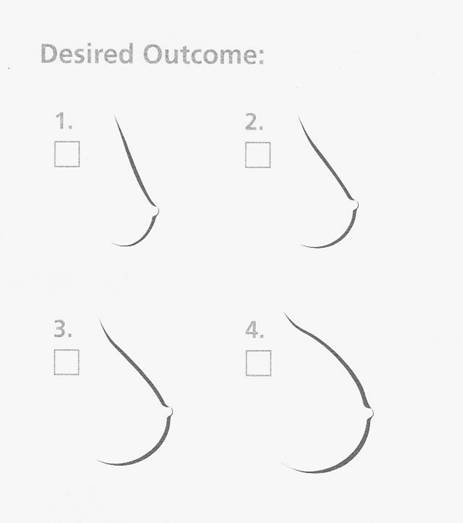
What shapes are available?
The majority of breast implants are round based with a variable height to allow different volumes to be achieved with the same rib cage size (breast base). However, some are oval and or shaped in profile. This allows the surgeon to have a number of options depending on the shape and type of result you are trying to achieve. Shaped implants are usually filled with the harder cohesive gel which holds its shape and therefore there is maximum benefit from the shaped implant (also called anatomical implants). The risk of a shaped implant is that if it moves around after positioning, it can leave an unsatisfactory result. However, there are situations where there is definite benefit in using a shaped implant. If you do require a shaped implant you may find these are more expensive and will add an extra cost to your surgery.
IMPLANT PLACEMENT
Where is it put?
Implants can be positioned under the breast tissue (subglandular) or under the pectoralis major muscle (subpectural). They are also very occasionally put under 2 layers of muscle (true submuscular placement). The choice of position depends on your body shape and the result you wish to achieve.
Most ladies requesting augmentation are fairly thin and wish to achieve a natural looking result. If implants are simply placed under a small breast in a thin lady, the top edge of the implant is very visible through the skin and the appearance is very artificial.
If the skin thickness is greater or the breast that is to be augmented is larger then it is possible to put an implant just under the breast and achieve a natural look. In a thin lady the most natural result is achieved by placing the implant partly under the breast but also tucking the implant under the bottom of the pectoralis major muscle. This hides the top of the implant and gives a more natural gentle rise over the breast. If the subpectoral placement is used it is a little more difficult to make the pocket for the implant to sit in, and there can be more bleeding afterwards. For this reason Miss Cubison always uses drains for this operation and suggests an overnight stay following the surgery. The subpectoral position also has a lower incidence of capsule formation than the subglandular position (see below).
Which scars will remain?
There are 3 options for scar placement although Miss Cubison prefers the inframammary fold approach which places the scar just under the breast. The final scar sits just on the new breast mound and is only visible when out of a bra or perhaps if your bikini rides up when playing beach volleyball! The scar is in the line that your bra makes and is therefore barely noticeable when it has settled down fully (after the first year to 18mths).
It is possible to put implants in using a cut around the nipple (periareolar). However, should you need to have your implants adjusted in the future it is not possible to use this approach and a second scar under the breast is needed. Miss Cubison therefore prefers to simply use the under the breast scar to start with and avoid the scar around the nipple.
It is also possible to place an empty saline implant under the breast using a cut in the armpit and keyhole techniques, and then inflate the implant when it is in position. This is not an operation that Miss Cubison is happy to perform and you would need to investigate other surgeons if you would like to consider this.
RISKS OF SURGERY
Any surgery has associated risks. Although a general anaesthetic is very safe there are still a small number of people who have problems with the anaesthetic itself. Other general risks include clots in the legs (deep vein thrombosis or DVT) and in the lungs (pulmonary embolus or PE). These problems are not commonly associated with Breast Augmentation but can occur.
Scars.
Your scars will usually be placed under the breast and gradually mature to a pale pink colour. To start off with they will be red and lumpy and you can help them to mature more quickly using regular massage and silicone gel. The maturation process takes about 2 years, although you will see noticeable improvement after about 9mths.
Capsules
The term capsule is used to describe the scar that forms around the implant. All implants have a capsule but there is considerable variation between patients and also between different implants and where they are placed. Modern implants have a textured coating that discourages aggressive capsule formation and this is much less of a problem than it was 20 years ago. In most patients capsule formation happens slowly and over a number of years. The first symptoms are gradual hardening of the implant and subtle changes in shape. In the later stages a severe capsule is painful and the implants appear very tight and spherical. With early implants most patients developed significant capsules that required further surgery over a 5 or 10 year period and this was referred to as needing a ‘Change of implant’. However, it is not the actual implant that is the problem rather the scar that surrounds it. We do not change implants because they are too old or past their best before date, only if the capsule surrounding them is causing problems. These days with modern implants capsule formation is less of a problem and although there is a possibility that you will have problems in the future we hope that you will have many happy years with your implants. There is an association with chronic infection and smoking in capsule formation, although this is not the case in all patients, and there are some people who are unlucky and just make very severe capsules soon after their implants are put in. If you do develop hardening or discomfort in your breasts an operation can be carried out to divide the capsule and release or replace the implants, but this will only be done if you are having problems. Research suggests that implants placed under the muscle have less tendency to produce capsules. However, this may just be that they are deeper so you are less aware of the changes in texture associated with very early capsule formation.
Rupture
If you suffer an injury to the breast area it is possible to rupture a breast implant. This is usually associated with a fall off a horse or a road traffic accident where the seatbelt vigorously squashes the implant. The rupture can be painful and the implants feel different. The diagnosis is usually made with an MRI scan or ultrasound and the implants are usually replaced. If you have a soft gel or saline implant the contents spill into the surrounding capsule and the saline is reabsorbed resulting in loss of volume. The soft silicone gel usually remains inside the capsule and is unlikely to cause problems.
Infections
As the surface of your implant has a special texture to reduce capsule formation it is an ideal place for bacteria to hide. The blood in your blood vessels does not get into the implant shell and therefore any bacteria that lodge there are not killed by the body’s natural defence mechanisms and antibiotics given in your blood do not get to them either. If you do get an infection around your implant it may be necessary to remove the implant and leave the capsule empty to allow your body to clear the infection. This can mean a period of 6 months without an implant and although a rare occurrence it does occasionally happen and you need to understand the risk. The highest infection risk to your implants is the process of putting them in, we take great care during your surgery to minimise this risk and use antibiotics in the first few days to try and prevent bacteria colonising the implants to start with. Any infection especially things like tooth abscesses can result in bacteria in your blood stream and it is important that these are treated quickly to avoid the bacteria finding your implants and settling there. If you have any areas of infection on the day of surgery it may be necessary to postpone your operation to reduce the risk of infection of your implants. If you are undergoing dental treatment or other surgery try and complete this more than 2 weeks before you are scheduled to have your implants put in to minimise the risk.
Bleeding and Haematoma formation
Any operation causes some bleeding, and although the apparent bleeding is controlled during the operation there is often some bleeding after the surgery as blood vessels relax and new bleeding points become apparent. Implants placed under the breast involve less bleeding as there is not the need to separate the muscle layers on the chest wall and therefore drains may not be needed. In submuscular placement the risk of bleeding is greater and drains are therefore used to take away the blood and try to prevent this forming a collection around the implants. Even with drains there is a small risk of developing a collection of blood around the implant, called a haematoma. If this occurs the affected breast will swell up very quickly within hours of surgery and will usually need to be treated with another operation within the next 24hours. Small collections of blood are less of a problem but are associated with increased risk of infection and capsule formation so we do not remove the drains until they have stopped collecting blood stained fluid.
Asymmetry
Most ladies do not have two breasts that are exactly the same and rib cages are often asymmetrical. If you look in the mirror you may see a prominent rib or that one nipple points in a different direction from the other. This is totally normal but sometimes these differences suddenly become noticeable after you have had surgery and are looking critically in the mirror. The shape of your rib cage provides the base that your implants sit on and if you have a very curved chest wall your implants will sit slightly pointing sideways. This is perfectly normal and is very natural. If you had originally developed larger breasts they would also have been in this position. It is important to wear your supportive bra to keep the cleavage that you will be expecting post surgery and to help your implants settle in the best position.
Numbness
The nerves that supply your breast and nipple are stretched by this surgery and some are actually cut. It is common to have some numbness after implant surgery and some ladies have increased sensation or pins and needles for a short time. This should settle down as the nerves recover but occasionally the numbness does remain.
Mammography
It is possible to have safe screening for breast cancer after breast augmentation. However, special views are required to ensure that all the breast tissue is properly seen. Make sure that you tell the radiographer that you have had implants to make sure that you have the correct x-rays taken. Breast implants do not cause breast cancer, but do not stop it occurring either. Your natural breast tissue remains on the outside of the implants so you should still regularly examine yourself for lumps, and if you find anything that worries you, visit your GP or breast surgeon.
Breast Feeding
As the breast tissue is still attached to the nipple it is still possible to breast feed after implants. However, many ladies do not have adequate breast tissue to produce sufficient breast milk. Don’t worry about very small traces of silicone getting into your milk, the formula milk manufacturers actually add silicone to their milk to help it flow nicely through the bottle teat!